
CHHRP’s Letter to the Icelandic Members of Parliament and Our Support for Children’s Rights
March 20,2018
Alþingi
Kirkjustræti
150 Reykjavík
Efni: Umsögn um frumvarp til laga um breytingu á almennum hegningarlögum (bann við umskurði drengja), 148. löggjafarþing, 114. mál. nefndasvid@althingi.is
Ágæta Alþingi / Dear Members of the Parliament:
The Children’s Health & Human Rights Partnership (CHHRP) is a dedicated not-for-profit partnership of Canadian medical, legal, and ethics professionals working collaboratively towards ending forced non-therapeutic genital cutting of children in Canada. Our work is in accordance with the Canadian Charter of Rights and Freedoms and international human rights law.
We write today to respectfully request your support for the proposed restrictions on non-therapeutic male infant circumcision in Iceland. Our hope is that you will take a strong stand in favour of allowing males—when there is otherwise no immediate medical need—to decide upon and consent to circumcision at an age when they can fully understand the consequences. Such a stand would be consistent with the international movement of child protection advocates, especially paediatric and medical societies and children’s ombudspersons in Nordic countries, who recognize this issue as an important human rights concern.
Child Rights International Network have noted in their recent 2018 report “What Lies Beneath”
With the exception of female genital mutilation, which is rightly one of the most widely recognised and challenged harmful traditional practices, there are a number of other procedures that involve irreversibly altering children’s genitals through surgery for no justifiable medical reason. These are: sex assignment of intersex children, forced sterilisation of children with learning disabilities, and routine male
circumcision, all three of which remain legal in most countries around the world when performed on children. (p. 21-22)
Full Document
https://www.crin.org/sites/default/files/crin_report_2018_edition.pdf
We wish to refer you to the 2012 report from the International NGO Council on Violence against Children. This groundbreaking report identifies numerous harmful practices based on tradition, culture, religion or superstition that violate the rights of children and the Council explicitly includes male circumcision as one of these practices.
It is difficult to argue that circumcision of otherwise healthy children is not a medical, cultural or religious tradition and that many parental motivations for requesting infant or child circumcision can be considered superstitious or based on fear of the unknown. The International NGO Council on Violence against Children (2012) explained that these practices are “perpetrated through false beliefs about child development and the cause and treatment of ill-health. These may stem from religious edict or belief, or from tradition or superstition or in some cases be promoted by health practitioners” (p. 7). The latter is certainly the case in North America, where paediatric societies take ambiguous stands and fail to firmly reject any medical justification for newborn circumcision and who issue statements that ignore the functions, benefits, and natural development of the foreskin, while failing to identify the newborn’s inherent right to bodily integrity.
In specifically identifying male circumcision as a traditional practice that violates the rights of male children, the International NGO Council on Violence against Children (2012) stated that “non-consensual, non-therapeutic circumcision of boys, whatever the circumstances, constitutes a gross violation of their rights, including the right to physical integrity, to freedom of thought and religion and to protection from physical and mental violence” (p. 22).
The International NGO Council on Violence against Children advised that circumcision and the other identified harmful practices
…should be effectively prohibited, when necessary explicitly, with particular attention to ensuring there are no provisions enabling parents or others to consent to/authorise such harmful practices; that prohibition is upheld explicitly in states with multiple legal systems including customary and/or religious law; that prohibition extends effectively not only to direct perpetrators but to those facilitating, arranging or offering the child for these practices. (2012, p. 46)
Full Document
http://srsg.violenceagainstchildren.org/sites/default/files/documents/docs/InCo_Report_15Oct.pdf
It has become increasingly clear that Nordic countries are taking seriously their pledge to protect children as well as their international treaty commitments regarding this group of vulnerable citizens. Their medical associations, child welfare agencies, and some legislative bodies reject the promotion of circumcision of otherwise healthy children, especially when such promotion is done by medical professionals and associations. We at CHHRP believe that your duty to children extends to the introduction of Icelandic law that explicitly identifies the right of all children to physical integrity and eventual self-determination and prohibits all forms of non-therapeutic genital cutting.
CHHRP has learned that there may have been attempts from one or more representatives of the United States of America government to influence the Icelandic Althingi on this issue. We are deeply concerned by this allegation, in light of the fact that the United States is the only nation in the world which has refused to ratify the United Nations Convention on the Rights of the Child (UNCRC). Furthermore, the United States’ national paediatric medical organization, the American Academy of Pediatrics (AAP), was publicly condemned by international paediatric authorities for its shoddy 2012 statement that failed to recognize the functions of the foreskin, the medical ethics involved in non-therapeutic circumcision, and the important human rights that are violated by those who circumcise otherwise healthy children. We direct you to one such rebuke signed by 38 physicians from 16 European nations as well as Canada.
Full Document: http://pediatrics.aappublications.org/content/early/2013/03/12/peds.2012-2896.full.pdf+html
SUMMARY
Iceland has always been a leader in the international arena when it comes to recognizing human rights — in some cases long before many other nations. We look forward to seeing this trend continue with the enactment of legislation that ensures that all Icelandic children are protected from non-therapeutic genital cutting.
Respectfully submitted,
Dr. Christopher Guest, MD, FRCPC, Medical Director
Dr. Ali A. Rizvi, MD, Advisory Board Member
Dr. Arif Bhimji, MD, Advisory Board Member
Dr. Cameron Bowman, MD, FRCSC, Advisory Board Member
Dr. Tracy Cassels, BA, MA, PhD, Advisory Board Member
Steven Caswell, JD, Advisory Board Member
Brian Moher, LLB, Advisory Board Member
Layli Samson, JD, Advisory Board Member
Monica Zamfir, JD, Advisory Board Member
Kira Antinuk, RN, BScN, MN, Nursing Director
Correspondence to the Canadian Paediatric Society Male Infant Circumcision Policy Committee:
10 February 2015
Canadian Paediatric Society
2305 St. Laurent Blvd
Ottawa, ON K1G 4J8
Attn: Fetus and Newborn Committee
cc. Dr. Robert Moriartey, MD, Canadian Paediatric Society President
Dear Colleagues,
As we await the Canadian Paediatric Society’s expected policy statement on neonatal circumcision, we wish to inform you of an important recent development.
You are no doubt aware that in December 2014 the U.S. Centers for Disease Control (CDC) inexplicably decided that they needed to draft recommendations to inform expectant parents about the benefits and risks of newborn circumcision, as well as offering guidance to adolescent and adult males about the procedure. The draft was titled “Recommendations for Providers Counseling Male Patients and Parents Regarding Male Circumcision and the Prevention of HIV Infection, STIs, and other Health Outcomes”.
To its credit, the CDC opened the draft recommendations to public comment for a period of 45-days, terminating on 16 January 2015.
What you may not be aware of is the following:
-
- The CDC received approximately 2,840 comments. Among the comments received from individuals and organizations, 97% opposed the CDC recommendations. Only 2% of comments expressed support, and 1% could be considered neutral. The comments are logged here: http://cdc.intactivist.net
- Some of the more salient responses from ethicists, attorneys and human rights NGOs are found here: http://www.circinfo.org/Centers_for_Disease_Control.html
- The Children’s Health & Human Rights Partnership provided its comments, which we provide to you as an attachment to this letter and may also be found here:
http://www.regulations.gov/#!documentDetail;D=CDC-2014-0012-1138 - The CDC requested the highly-respected U.S. pediatrician Robert S. Van Howe, M.D. to provide a critique of the recommendations. Dr. Van Howe has now submitted his 208-page critique— containing 1,351 references—which can be reviewed here:
https://www.academia.edu/10553782
We presume that the CPS is still formulating its new statement on this matter and wanted to bring these matters to your attention in a timely manner.
In unity for the children,
Dr. Christopher L. Guest, MD, FRCPC Medical Director
Kira Antinuk, RN, BScN Nursing Director
Tim Hammond Outreach Director
David Saving Technical Director
Dr. Arif Bhimji, MD Advisory Board Member
Dr. Cameron Bowman, MD, FRCSC Advisory Board Member
Dr. Kaleb Montgomery, HBSc, DTCM Advisory Board Member
Jessica Forbes, RM Advisory Board Member
Kerstin Helén, RN, RM, BScN Advisory Board Member
Tony Chacon, RN, BSN, MN(c) Advisory Board Member
Geoffrey T. Falk, BSc, MA Advisory Board Member
Tracy Cassels, BA, MA, PhD(c) Advisory Board Member
Dr. Ali A. Rizvi, MD Advisory Board Member
Jennifer Pinch, RN, BScN, CD(DONA) Advisory Board Member
Attachment
PUBLIC COMMENTS PROVIDED BY
THE CHILDREN’S HEALTH & HUMAN RIGHTS PARTNERSHIP ON DRAFT RECOMMENDATIONS BY
THE U.S. CENTERS FOR DISEASE CONTROL REGARDING MALE CIRCUMCISION
The Children’s Health & Human Rights Partnership is Canada’s premiere not-for-profit group of health care professionals and scholars devoted to protecting the genital health and human rights of Canada’s male, female, and intersex children. We realize that CDC recommendations can influence some Canadians and are pleased to provide public comment on your draft recommendations concerning male circumcision.
In Canada, the practice of infant circumcision was once as widespread as it is now in the U.S. For the past several decades, however, none of our provinces or private health plans pay for infant circumcision, since there is no medical necessity to perform surgery on a newborn male’s healthy penis. That’s why hospital circumcision rates here are less than 10%, compared to the U.S. national average of around 50%.
Like parents in most of the world, we don’t view our newborn sons’ genitals as being somehow defective and in need of immediate surgical improvement. We trust in our parental abilities to teach our children proper hygienic behaviours as well as adoption of safer sex practices to protect themselves from sexually transmitted infections, all while still enjoying intact genitals.
That’s why the vast majority of our intact boys and men do not suffer the laundry list of maladies described in your draft recommendations.
We invite you to review the attached report from the International NGO Council on Violence against Children (2012), which states, “…non-consensual, non-therapeutic circumcision of boys, whatever the circumstances, constitutes a gross violation of their rights, including the right to physical integrity, to freedom of thought and religion and to protection from physical and mental violence” (p. 22). The report also notes, “The WHO review quoted three randomized controlled trials suggesting that circumcision reduces the risk of acquiring HIV infection in males. But this potential health benefit does not override a child’s right to give informed consent to the practice. The decision to undertake circumcision for these reasons can be deferred to a time where the risk is relevant and the child is old enough to choose and consent for himself” (p. 22).
Canadians are very much like Americans in many respects, except that Canada (like every other nation in the world except the U.S.) has ratified the U.N. Convention on the Rights of the Child. Article 24 of the Convention calls on signatory nations to protect their children from traditional practices prejudicial to their health and human rights. Infant circumcision exposes children to unnecessary risk and, by the CDC’s own admission, is a social custom and therefore a traditional practice covered in the Convention.
We call on the CDC to revise its recommendations that appear to condone the practice of infant circumcision and to include unequivocal language urging health professionals to reassure parents that the vast majority of intact men and boys do not suffer foreskin ailments and that in those rare occasions when a medical problem might arise during childhood, it can be conservatively treated medically, and only as a last resort surgically.
They can also offer reassurance that while parents are responsible for making a myriad of decisions on behalf of their child (vaccinations, nutrition, etc), circumcision is not one they need concern themselves with. Indeed, such an intimate personal decision is best left to each individual male to make when he is of an age to have his own reasons (if any), and to understand and give fully informed consent. To usurp such a decision is not within a parent’s responsibilities and is a violation of their child’s inherent human rights.
Correspondence to the Canadian Paediatric Society Male Infant Circumcision Policy Committee:
19 May 2014
To the members of the Canadian Paediatric Society Male Infant Circumcision Policy Committee
cc. Dr. Andrew Lynk, MD, Canadian Paediatric Society President
The Children’s Health & Human Rights Partnership (CHHRP) is Canada’s first dedicated not-for-profit partnership of medical, legal, and ethics professionals working alongside concerned citizens towards ending forced non-therapeutic genital cutting of children in Canada. Our work is in accordance with the Canadian Charter of Rights and Freedoms and international human rights law.
We write today to inform you of important developments surrounding the practice of infant male circumcision which should be seriously considered when formulating any future policy statements on the practice in Canada. We offer this with the hope that the Canadian Paediatric Society will take a strong stand in favour of allowing males—when there is otherwise no immediate medical need—to decide upon and consent to circumcision at an age when they can fully understand the consequences.
Such a stand would be consistent with the international movement of child protection advocates, especially paediatric and medical societies and children’s ombudspersons in Europe, who recognize this issue as an important human rights concern.
We enclose for your benefit a copy of the 2012 report from the International NGO Council on Violence against Children. This groundbreaking report identifies numerous harmful practices based on tradition, culture, religion or superstition that violate the rights of children.
While we encourage you to read the entire report for contextual reasons, we wish to draw your attention to those sections we believe are relevant to the present discussion of neonatal circumcision.
Page 7 lists general categories of rights violations based on tradition, culture, religion and superstition. It is difficult to argue that circumcision of otherwise healthy newborns is not a medical, cultural or religious tradition and that many parental motivations for requesting newborn circumcision can be considered superstitious or based on fear of the unknown, e.g., “My uncle had to be circumcised as an adult so we might as well do it to our son now” or “My son will be psychologically harmed if he doesn’t look like his circumcised father or the other boys”.
The report goes on to state (bolding is ours): “The list includes a number of practices perpetrated through false beliefs about child development and the cause and treatment of ill-health. These may stem from religious edict or belief, or from tradition or superstition or in some cases be promoted by health practitioners.”
This is the case especially in North America, where paediatric societies take ambiguous stands and fail to firmly reject any medical justification for newborn circumcision and who issue statements that ignore the functions, benefits, and natural development of the foreskin, while failing to identify the newborn’s inherent right to bodily integrity. You will take note that the practice of male circumcision is specifically identified on pages 21 and 22 as a traditional practice that violates the rights of male children (to bodily integrity). The report states that “non- consensual, non-therapeutic circumcision of boys, whatever the circumstances, constitutes a gross violation of their rights, including the right to physical integrity, to freedom of thought and religion and to protection from physical and mental violence.”
The report also recognizes that “There are now substantial established campaigns against non-therapeutic, non-consensual circumcision of boys and growing support to end it, particularly within the medical community.” The rest of the paragraph from which this excerpt was taken, we believe, is mandatory reading for any paediatric association that claims to have its child patients’ best interests at heart.
Page 47 of the report asserts that health practitioners should be encouraged to work actively to eliminate these harmful practices as parts of their codes of ethical conduct. We at CHHRP assert that this duty to child patients extends to the issuance of a neonatal circumcision policy that explicitly identifies the right of the child to physical integrity and eventual self-determination.
It has become increasingly clear that Europeans are taking seriously their pledge to protect children as well as their international treaty commitments regarding this group of vulnerable citizens. Their medical associations, child welfare agencies, and some legislative bodies reject the promotion of circumcision of otherwise healthy children, especially when such promotion is done by medical professionals and associations.
The American Academy of Pediatrics (AAP) has been publicly condemned by international paediatric authorities for its shoddy 2012 statement that failed to recognize the functions of the foreskin, the medical ethics involved in non-therapeutic circumcision, and the important human rights that are violated by those who circumcise otherwise healthy children. We direct you to one such rebuke signed by 38 physicians from 16 European nations, and Canada’s own Dr. Noni MacDonald.
Source: http://intaction.org/circumcision-policy-denounced/
Full Document: http://pediatrics.aappublications.org/content/early/2013/03/12/peds.2012-2896.full.pdf+html
As further evidence of the cultural bias and personal and professional ignorance of AAP Task Force members on this matter, in October 2013 at the 20th Pitts Lectureship in Medical Ethics at the Medical University of South Carolina in Charleston, South Carolina two members of the AAP Task Force on Circumcision were asked by a member of the audience to identify the functions of the foreskin. Task Force member Dr. Michael Brady stated “I don’t think anyone knows the functions of the foreskin” and later reiterated “Nobody knows the functions of the foreskin.”
It deeply concerns us to report that the bias does not end there. Dr. Andrew Freedman, one of the AAP circumcision policy task force members, when asked if he had a son and whether he had him circumcised, was quoted as saying: “Yes, I do. I circumcised him myself on my parents’ kitchen table.” We at CHHRP certainly hope the CPS has taken the necessary steps to guard against such blatant conflicts of interest amongst the members of its Male Infant Circumcision Policy Committee.
Source: http://www.thejewishweek.com/features/new-york-minute/fleshing-out-change-circumcision
We also note that much media attention has been paid recently to a recent review that attempts to equate neonatal circumcision with vaccination. Any clear-thinking individual can see the many ways in which this is a false equivalency; however, if left unchecked, this logically unsupportable notion may gain traction among the public. We hope that any future CPS statement on circumcision will refute such attempts to conflate these two practices.
Source: http://www.ctvnews.ca/health/circumcision-should-be-seen-in-the-same-light-as-childhood-vaccination- study-1.1757650#ixzz2xkx6ATBP
SUMMARY
Canada has always been a leader in the international arena when it comes to recognizing human rights — in many cases long before our immediate neighbours to the South. We look forward to a forthcoming update from the CPS on this topic and sincerely hope that the update will not embarrass Canadians by merely parroting the AAP statement, but will be a document that all Canadians can be proud of by progressively incorporating the important issues described in the enclosed report.
In unity for the children,
Dr. Christopher L. Guest, MD, FRCPC Medical Director
Kira Antinuk, RN(P), BSN Nursing Director
Tim Hammond Outreach Director
David Saving Technical Director
Dr. Arif Bhimji, MD Advisory Board Member
Dr. Cameron Bowman, MD, FRCSC Advisory Board Member
Dr. Kaleb Montgomery, HBSc, DTCM Advisory Board Member
Jessica Forbes, RM Advisory Board Member
Kerstin Helén, RN, RM, BScN Advisory Board Member
Tony Chacon, RN, BSN, MN(c) Advisory Board Member
Geoffrey T. Falk, BSc, MA Advisory Board Member
Tracy Cassels, BA, MA, PhD(c) Advisory Board Member
Correspondence to the Canadian AIDS Society:
30 September 2013
Dear Monique Doolittle-Romas,
The Children’s Health & Human Rights Partnership (CHHRP) is Canada’s first dedicated not-for-profit partnership of medical, legal, and ethics professionals working alongside concerned citizens towards ending forced non-therapeutic genital cutting of children in Canada. We write today to share our concerns regarding your policy on male circumcision and HIV.
In particular, we ask the Canadian AIDS Society (CAS) to incorporate two issues into your male circumcision policy:
1) The methodologically flawed nature of studies that allegedly support male circumcision in the campaign against HIV
2) CAS male circumcision policy implications
Methodology
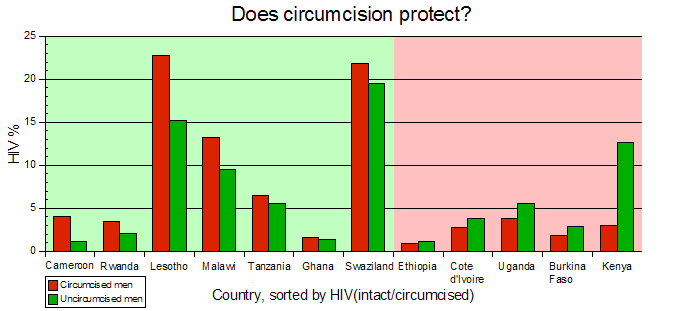
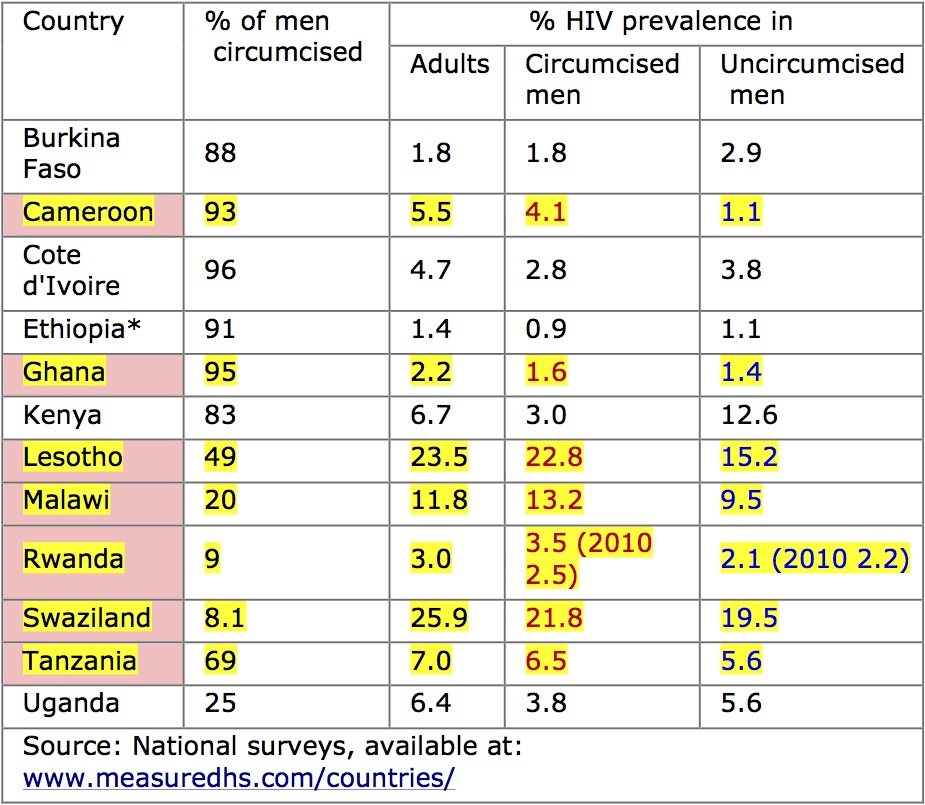
While many well-intentioned health organizations have cited the African circumcision trials as reliable evidence that male circumcision is an effective tool in the fight against HIV/AIDS, these studies are misleading. For example, assuming the quoted 50-60% risk reduction was scientifically valid, this is a “relative risk” reduction, as opposed to an “absolute risk” reduction. The absolute risk reduction in these studies was 1.31% – a significantly smaller number than the figure touted publicly.123 (Please see Appendix A for an explanation of relative and absolute risk reduction). This misleading and unscientific data manipulation falsely implies that male circumcision is effective at preventing HIV/AIDS. Many men may believe that they no longer need to use condoms after undergoing circumcision. Furthermore, these African trials contradict larger demographic trends with respect to circumcision and HIV/AIDS prevalence. For instance, the United States has a high circumcision rate but also has a significantly higher rate of heterosexual HIV transmission than other countries where circumcision is very rare. Collectable data from African countries shows circumcising countries also have a higher prevalence for HIV/AIDS, (see Appendix B). Correct and consistent use of condoms reduces HIV transmission by an absolute risk reduction of 80% 4 – far higher than the alleged 1.31% absolute risk reduction for male circumcision. Effective and ethical prevention strategies should emphasize correct condom usage, which is still required even after circumcision.
As Boyle, G. J., & Hill, G. stated, “While the ’gold standard’ for medical trials is the randomised, double-blind, placebo-controlled trial, the African trials suffered design and sampling problems including; problematic randomisation and selection bias, inadequate blinding, lack of placebo-control (male circumcision could not be concealed), inadequate equipoise, experimenter bias, attrition (673 drop-outs in female-to-male trials [7% drop out rate]), not investigating male circumcision as a vector for HIV transmission, not investigating non-sexual HIV transmission, as well as lead-time bias, supportive bias (circumcised men received additional [safe sex] counselling sessions), participant expectation bias, and time-out discrepancy (restraint from sexual activity only by circumcised men).”5 Many other scientific papers have also been highly critical of the HIV trials as a method for HIV/AIDS reduction.6789
CAS Male Circumcision Policy Implications
The CAS states in its circumcision policy statement, “Ultimately, it is another prevention option that should be available to those who choose it as such”. This begs a serious ethical and human rights question of whether the parent has the right to choose or whether consent must come from the individual to whom the genitals belong, once he reaches an appropriate age. It is the individual who must live with the permanent physical, sexual, and psychological effects of the surgery, as well as any additional surgical complications. For further information, please see the results of the Global Survey of Circumcision Harm at www.circumcisionharm.org
We receive frequent reports that many of these African circumcision programs, intended for consenting adult men, are in fact influencing North American parents to impose forced circumcision on their newborn male infants. Since these children will not become sexually active for many years, subjecting them to a permanent surgical alteration, in a misguided attempt to prevent future disease, violates their personal autonomy and robs them of their right to physical integrity as guaranteed in the Canadian Charter of Rights and Freedoms.
Canadian human rights law and treatises maintain that all children have equal protection under the law. These include:
The Universal Declaration of Human Rights (UDHR), adopted by Canada in 1948 (http://www.un.org/en/documents/udhr/)
The United Nations Convention on the Rights of the Child (CRC) ratified by Canada in December 1991. Specifically, Article 24.3 declares, “State Parties shall take all effective and appropriate measures with a view to abolishing traditional practices prejudicial to the health of children.” (http://www.un.org/documents/ga/res/44/a44r025.htm)
The Canadian Charter of Rights and Freedoms, enshrined in the Canadian constitution in 1982 (http://laws-lois.justice.gc.ca/eng/Const/page-15.html)
Any form of non-consensual female genital cutting—equal to or less invasive than male infant circumcision, including removal of the female prepuce—for any reason, including the potential to reduce vulvar cancer or sexually transmitted diseases, has been illegal in Canada since 1997.1011 Circumcision of otherwise normal healthy boys is in direct conflict with gender equality rights spelled out in the above documents.
The Valid Function of the Foreskin
“The prepuce [foreskin] is an integral, normal part of the external genitalia that forms the anatomical covering of the glans penis and clitoris… The prepuce is richly innervated, erogenous tissue.”12 It also serves an important mechanical function, providing a linear bearing mechanism during sexual intercourse.1314 For further information on the form and function of the penis and the mechanics of intercourse please visit the cited references.
Respect for a child’s developing sexuality, regardless of gender, is recognized in the 1997 Valencia Declaration of Sexual Rights adopted by the XIII World Congress of Sexology, which states:
“We urge that societies create the conditions to satisfy the needs for the full development of the individual and respect the following sexual rights: …The right to autonomy, integrity and safety of the body. This right encompasses control and enjoyment of our own bodies, free from torture, mutilation and violence of any sort.”15
Summary
CHHRP invites the CAS to join thousands of people around the world in efforts to define, expand, and protect human rights in health relevant settings—such as sexual rights and health—and to uncover substantial inconsistencies in health thinking. One such inconsistency is the unquestioned respect for a female child’s right to genital integrity and autonomy that has thus far been ignored for the male child.
It is our hope that the CAS will recognize that male circumcision is not an effective tool in the fight against HIV/AIDS. We also hope that the CAS recognizes the human rights and possible Canadian legal implications of suggesting male circumcision as part of a HIV/AIDS prevention strategy. We look forward to a continuing dialogue with the CAS.
Respectfully submitted by,
Christopher L. Guest M.D., F.R.C.P.C.
Medical Director, Children’s Health & Human Rights Partnership
1300 King St E PO Box 31011
Kingsway Village PO
Oshawa, ON L1H 8N9
References
1 Bailey, R.C., Moses, S., Parker, C.B., Agot, K., Maclean, I., Krieger, J.N., et al. Male circumcisi1on for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet 2007; 369: 643-56 doi: 10.1016/S0140-6736(07)60312-2 pmid: 17321310.
2 Auvert, B., Taljaard, D, Lagarde, E., Sobngwi‐Tambekou, J., Sitta, R., & Puren, A. (2005). Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: the ANRS 1265 Trial. PLoS medicine, 2 (11), e298.
3 Gray, R. H., Kigozi, G., Serwadda, D., Makumbi, F., Watya, S., Nalugoda, F., et al. (2007). Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. The Lancet, 369 (9562), 657‐666.
4 Wilton, J. (2013). Condoms: Tried, tested and true? From CATIE: Canada’s source for HIV and hepatitis C information: http://www.catie.ca/pif/spring‐2013/condoms‐tried‐tested‐and‐true
5 Boyle, G. J., & Hill, G. (2011). Sub‐Saharan African randomised clinical trials into male circumcision and HIV transmission: methodological, ethical and legal concerns. Journal of law and medicine, 19 (2), 316.
6 Green, et al., (2010). Male Circumcision and HIV Prevention: Insufficient Evidence and Neglected External Validity. Am J Prev Med 2010;39(5):479–482
7 Darby, R. & Van Howe, R. (2011), Not a surgical vaccine: there is no case for boosting infant male circumcision to combat heterosexual transmission of HIV in Australia. Australian and New Zealand Journal of Public Health, 35: 459–465. doi: 10.1111/j.1753‐ 6405.2011.00761.x
8Frisch, M., Aigrain, Y., Barauskas, V., Bjarnason, R., Boddy, S. A., Czauderna, P., et al. (2013). Cultural bias in the AAP’s 2012 technical report and policy statement on male circumcision. Pediatrics , 131 (4), 796‐800.
9Van Howe, R. S. & Storms, M. R. (2011). How the circumcision solution in Africa will increase HIV infections. Journal of Public Health in Africa 2011; 2:e4 doi: 10.4081/jphia.2011.e4
10 Government of Canada. (2013, July 15). Justice Laws Website. From Criminal Code s 266 Assault: http://laws‐lois.justice.gc.ca/eng/acts/C‐46/page‐131.html#docCont
11Parliament of Canada. (n.d.). BILL C‐27. From Parliament of Canada: http://www.parl.gc.ca/HousePublications/Publication.aspx?DocId=2329459&File=16
12 Cold, C. J., & Taylor, J. R. (1999). The prepuce. BJU international , 83 (S1), 34‐44.
13 Anatomy of the Penis, Mechanics of Intercourse (http://www.cirp.org/pages/anat/)
14 Animation on the foreskin linear bearing mechanism during sexual intercourse (http://www.circumstitions.com/Works.html)
15 World Association for Sexology. (2007, November). Valencia Declaration on Sexual Rights.
Appendix A
What does Relative risk reduction and Absolute risk reduction mean?
The misleading Relative Risk Ratio
Newspapers like big numbers and eye-catching headlines. They need miracle cures and hidden scares, and small percentage shifts in risk will never be enough for them to sell readers to advertisers (because that is the business model). To this end they pick the single most melodramatic and misleading way of describing any statistical increase in risk, [Or “Reduction” in the case of circumcision and HIV] which is called the ‘relative risk increase’.
Let’s say the risk of having a heart attack in your fifties is 50 per cent higher if you have high cholesterol. That sounds pretty bad. Let’s say the extra risk of having a heart attack if you have high cholesterol is only 2 per cent. That sounds OK to me. But they’re the same (hypothetical) figures. Let’s try this. Out of a hundred men in their fifties with normal cholesterol, four will be expected to have a heart attack; whereas out of a hundred men with high cholesterol, six will be expected to have a heart attack. That’s two extra heart attacks per hundred. Those are called ‘natural frequencies’.
Natural frequencies are readily understandable, because instead of using probabilities, or percentages, or anything even slightly technical or difficult, they use concrete numbers, just like the ones you use every day to check if you’ve lost a kid on a coach trip, or got the right change in a shop. Lots of people have argued that we evolved to reason and do maths with concrete numbers like these, and not with probabilities, so we find them more intuitive. Simple numbers are simple.
The other methods of describing the increase have names too. From our example above, with high cholesterol, you could have a 50 per cent increase in risk (the ‘relative risk increase’); or a 2 per cent increase in risk (the ‘absolute risk increase’); or, let me ram it home, the easy one, the informative one, an extra two heart attacks for every hundred men, the natural frequency.
As well as being the most comprehensible option, natural frequencies also
contain more information than the journalists’ “relative risk increase”.
Excerpt from “Bad Science” by Ben Goldacre, Fourth Estate, London (2008), p 256-9
Appendix B
Male circumcision and HIV prevalence in Africa
“There appears to be no clear pattern of association between male circumcision and HIV prevalence. In 8 of 18 countries with data, as expected, HIV prevalence is lower among circumcised men, while in the remaining 10 countries HIV prevalence is higher among circumcised men…
Findings from the 18 countries with data present a mixed picture of the association between male circumcision and HIV prevalence. In eight of the countries (Burkina Faso, Cambodia, Côte d’Ivoire, Ethiopia, Ghana, India, Kenya, and Uganda), HIV prevalence is higher among men who are not circumcised, although the difference between circumcised and non-circumcised men is slight, except in Kenya, where the difference is substantial (HIV prevalence of 11.5 percent for non-circumcised men compared with 3.1 percent for circumcised men). In 10 of the countries (Cameroon, Guinea, Haiti, Lesotho, Malawi, Niger, Rwanda, Senegal, Tanzania, and Zimbabwe) HIV prevalence is higher among circumcised men.”
United States Agency for International Development (USAID) February 2009
Correspondence to the Canadian Paediatric Society:
17 February 2013
To the members of the Canadian Paediatric Society Male Infant Circumcision Policy Committee
The Children’s Health & Human Rights Partnership (CHHRP) is Canada’s first dedicated not-for-profit partnership of medical, legal, and ethics professionals working alongside concerned citizens towards ending forced non-therapeutic genital cutting of children in Canada. We write today to share with you our position and resources as you revise the CPS policy on infant male circumcision.
INTRINSIC VALUE OF THE MALE PREPUCE
The foreskin has been identified to have protective, sensory and sexual functions. Respected Canadian pathologist and medical researcher Dr. John R. Taylor stated:
“The prepuce is a specialized, specific erogenous tissue in both males and females. Therefore, surgical excision should be restricted to lesions that are unresponsive to medical therapy, such as lichen sclerosis of the penis (balanitis xerotica obliterans) or vulva, which is unresponsive to other therapies (e.g. topical clobetasol, intralesional corticosteroids, topical testosterone propionate ointment, etretinate, and carbon dioxide or laser vaporization). Preputial plasty should be considered in place of circumcision whenever possible, so as to preserve the corpuscular sensory receptors, dartos muscle, penile mucosa and complete function of the penis, while avoiding abnormal exposure and keratinization of the glans penis. The complex anatomy and function of the prepuce, along with the fused prepuce/glans penile mucosa in the immature penis, dictates that neonatal circumcision be strictly avoided.”1
We urge the CPS committee to thoroughly consider Dr.Taylor’s contributions in documenting the value and functional purposes of the male foreskin. Numerous recent studies confirm the fact that male circumcision causes sexual dysfunctions for men and negative consequences for their partners. A recent study from Belgium concluded:“The foreskin is more sensitive than the uncircumcised glans mucosa, which means that after circumcision genital sensitivity is lost. In the debate on clitoral surgery the proven loss of sensitivity has been the strongest argument to change medical practice. In the present study there is strong evidence on the erogenous sensitivity of the foreskin. This knowledge hopefully can help doctors and patients in their decision on circumcision for non-medical reason. This study confirms the importance of the foreskin for penile sensitivity, overall sexual satisfaction, and penile functioning. Furthermore, this study shows that a higher percentage of circumcised men experience discomfort or pain and unusual sensations as compared with the uncircumcised population.” 2
IMMEDIATE RISKS AND ADVERSE LONG-TERM CONSEQUENCES
There is documented physiological and psychological damage due to the foreskin unnecessarily being removed. Although not reimbursed under provincial health plans, male infant circumcision by pro-circumcision entrepreneurs remains an all too commonly performed surgery in Canada, with rates varying regionally.3 The typical rationale given for this non-therapeutic surgery is parental preference. 4
There are a number of risks documented in the literature, ranging from hemorrhage to infection to meatal stenosis to death. The psychological consequences of an early circumcision 5 6 7 remain largely undiscussed in the statements of medical societies and have not been incorporated into their recommendations.
In addition, a growing number of adult men believe they were harmed by a circumcision they did not choose, as evidenced by the results of the Global Survey of Circumcision Harm.(see www.CircumcisionHarm.org.)
CANADA’S HUMAN RIGHTS OBLIGATIONS
Children’s human rights are violated when the foreskin is removed unless for truly emergent reasons. No medical organization in the world recommends routine male infant circumcision and a number of national medical organizations strongly condemn the practice 8. While discussion in Canada and the United States appears to still be focused on questionable attempts to justify non-therapeutic genital cutting, countries in Europe, particularly in Scandinavia, have shifted the debate towards the true crux of the issue: human rights and equality. Canada has a long history of acting with leadership and courage to ensure that human rights are safeguarded. John Peters Humphrey OC, a Canadian legal scholar, was the principal drafter of what became the Universal Declaration of Human Rights. In 1991, Canada became a signatory to the United Nations Convention on the Rights of the Child. Male infant circumcision violates this and other human rights legal documents.9 These include:
- The Universal Declaration of Human Rights (UDHR), adopted by Canada in 1948 (http://www.un.org/en/documents/udhr/)
- The United Nations Convention on the Rights of the Child (CRC) ratified by Canada in December 1991. Specifically, Article 24.3 declares that “State Parties shall take all effective and appropriate measures with a view to abolishing traditional practices prejudicial to the health of children.” (http://www.unicef-irc.org/portfolios/crc.html)
- The Canadian Charter of Rights and Freedoms, enacted by Canada in 1982 (http://laws-lois.justice.gc.ca/eng/Const/page-15.html)
Under these documents, as well as Canadian criminal law, any form of non-consensual female genital cutting—equal to or less invasive than male infant circumcision, including removal of the female prepuce—has been illegal in Canada since 1997 for any reason, including religion, culture or parental choice. Circumcision of otherwise normal healthy boys is in direct conflict with gender equality rights spelled out in the above documents.
In 2015, boys that were circumcised after this enactment will become adults and could launch Charter-based lawsuits against their circumcisers for violating their human rights. This point requires serious consideration.
It is our sincere hope that, with regard to the social custom of infant male circumcision, the CPS will support the legal and treaty obligations of Canada’s governmental and non- governmental agencies to protect human rights as defined in these documents.
SUMMARY
CHHRP invites the CPS to join us and thousands of people around the world in efforts to define, expand, and protect human rights in health relevant settings—such as sexual rights and health—and to uncover substantial inconsistencies in health thinking. One such inconsistency is the unquestioned respect for a female child’s right to genital integrity and autonomy that has heretofore been ignored for the male child. It is our hope to begin a dialogue with the CPS with the mutual goal of promoting the health and human rights of children in Canada.
For future CPS infant circumcision statements, CHHRP encourages the CPS to adopt the following positions:
- the recognition of the protective, sensory and sexual functions of the male prepuce and education on proper care including the associated harm from forcible retraction.
- the recognition that children’s human rights are violated when the foreskin is unnecessarily removed and that there is documented harm caused by it’s loss.
- the discouragement of religious or cultural surgery without medical indication while adopting the World Medical Association’s Declaration of Geneva (2006),which states “I will not use my medical knowledge to violate human rights and civil liberties, even under threat.”
Respectfully submitted by the Co-Founders,
Christopher L. Guest M.D., F.R.C.P.C.
Kira Antinuk, R.C.A., B.S.N.S. (University of Victoria)
David Saving
Tim Hammond
1300 King St E PO Box 31011 Kingsway Village PO
Oshawa, ON L1H 8N9
cc. Richard Stanwick, Canadian Paediatric Society President
REFERENCES
1 Cold, C. J., & Taylor, J. R. (1999). The prepuce. BJU International, 83 Suppl 1(S1), 34-44. doi: 10.1046/j.1464-410x.1999.0830s1034.x
2 Bronselaer, G.A., Schober, J.M., Meyer-Bahlburg, H.F., T’sjoen, G., Vlietinck, R., Hoebeke, P.B.. (2013). Male circumcision decreases penile sensitivity as measured in a large cohort. BJU Int. doi: 10.1111/j.1464-410X.2012.11761.x.
3 Public Health Agency of Canada. (2009). Mothers’ voices: What women say about pregnancy, childbirth and early motherhood. Ottawa: Public Health Agency of Canada.
4 Elmore, J. M., Baker, L. A., & Snodgrass, W. T. (2002). Topical steroid therapy as an alternative to circumcision for phimosis in boys younger than 3 years. The Journal of Urology, 168 (4 Pt 2), 1746-1747. doi: 10.1016/S0022-5347(05)64404-7
5 Boyle, G.J., Goldman, R., Svoboda, J.S., et al. (2002). Male circumcision: pain, trauma and psychosexual sequelae. J Health Psychol 2002. 7329–343.
6 Taddio, A., Katz, J., Ilersich, A.L., Koren, G., (1997). Effect of neonatal circumcision on pain response during subsequent routine vaccination. Lancet 1997;349(9052):599-603.
7 Yilmaz, E., Batislam, E., Basar, M. M., & Basar, H. (2003). Psychological trauma of circumcision in the phallic period could be avoided by using topical steroids. International Journal of Urology: Official Journal of the Japanese Urological Association, 10(12), 651-656. doi: 10.1046/j.1442-2042.2003.00722.x
8 CIRP, (2012). Circumcision Policy Statements. Retrieved from http://www.cirp.org/library/ statements/ on 4 February 2012
9 Zavales, A., (1995). Introduction to the Urgent Human Rights Proposal (p. 11) in Universal Reproductive & Human Rights: Ordering Corrective Action against North American Circumcisers, Sloatsburg, NY
In 1996 the CPS presented the following conclusions in its Male Infant Circumcision Policy:
“There is evidence that circumcision results in an approximately 12-fold reduction in the incidence of UTI during infancy.”1
A recent Scandinavian study found that girls and boys have about the same incidence of UTI in the first year of life. While non-circumcised female children have a four times higher incidence of UTI in the first six years of life than non-circumcised male children, no special concern is manifested regarding this much higher rate of infection in females and surgery has not been proposed 2
“The incidence rate of the complications of circumcision reported in published articles varies, but it is generally in the order of 0.2% to 2%. Most complications are minor, but occasionally serious complications occur.”3
Williams & Kapila estimated a realistic complication rate of 2% to 10% 4. There is a need for good epidemiological data on the incidence of the surgical complications of circumcision, of the later complications of circumcision and of problems associated with lack of circumcision. We invite you to review the results of the Global Survey of Circumcision Harm for further information about long-term adverse outcomes.
“Evaluation of alternative methods of preventing UTI in infancy is required.”5
As documented in numerous studies, breastfeeding plays a central role in preventing UTIs and does not carry any of the risks of genital surgery. In addition, rooming-in facilitates colonization of the infant’s skin and mucosa with the mother’s own bacteria. The prepuce and other skin and mucosa of the infant should be specifically brought into contact with the mother’s own skin to initiate the child’s natural immunity by passing along her flora.6
“More information on the effect of simple hygienic interventions is needed.” 7
CHHRP members do receive anecdotal reports of physicians, nurses, and other healthcare providers instructing parents to retract the prepuce and clean underneath. This is an outdated practice which involves tearing the synechia, and potentially causing pain, skin tears, inflammation, and infection.
“Information is required on the incidence of circumcision that is truly needed in later childhood.”8
Denniston states: “Since the neonatal circumcision rate in Finland, where virtually every male wishes to preserve his foreskin, is zero, and since the risk of needing a late circumcision in Finland is one in 16,667, it follows that almost all of the circumcisions still being done in North America have no medical necessity, and in fact, are contraindicated.”9
“There is evidence that circumcision results in a reduction in the incidence of penile cancer and of HIV transmission. However, there is inadequate information to recommend circumcision as a public health measure to prevent these diseases.”10
The assumption that circumcision has prophylactic value against heterosexually transmitted HIV infections is mainly based on data collected in Sub-Saharan Africa, which are strongly doubted. The African HIV trials reveal a number of methodological weaknesses 11 and they contradict larger demographic trends in global HIV prevalence. For instance, the United States has a high prevalence of circumcision12, yet has a significantly higher rate of HIV infection compared with countries like Sweden and Japan where the prevalence of circumcision is very low13. HIV from men who had sex with men (MSM) is no different based on circumcision status14. Behavioural factors greatly overshadow any potential protective effect of circumcision and should be the focus of effective and ethical prevention strategies. Even if the African trials were scientifically valid, the evidence can not be applied to justify infant circumcision in countries where the incidence of heterosexual HIV transmission is low15
With regard to penile or cervical cancers, it is known that Human Papilloma Virus (HPV) is largely responsible, transmission of which can be effectively prevented by proper hygiene and the use of condoms. Additionally the recently released HPV vaccine, Gardasil, can play a major role in prevention against genital infections among sexually active men and women. All of these obviate the need for infant male circumcision.
“When parents are making a decision about circumcision, they should be advised of the present state of medical knowledge about its benefits and harms. Their decision may ultimately be based on personal, religious or cultural factors.”16
In 2010, the American Academy of Pediatrics issued a statement to its members suggesting that they honour the practice of performing clitoral nicking on female infants based on personal, religious, cultural or parental wishes. After a significant backlash from the medical community and the public, this statement was rescinded. We hope the CPS will give appropriate consideration to the same fundamental right to bodily integrity for male children that it accords to female children.
1 Canadian Paediatric Society, (1996). Neonatal circumcision revisited. Canadian Medical Association Journal 1996: 154(6):769-780
2 Brandström, P., Jodal, U., Sillén, U., Hansson, S., Institute of Clinical Sciences, Section for the Health of Women and Children, Department of Pediatrics, Göteborgs universitet, Sahlgrenska akademin. (2011). The swedish reflux trial: Review of a randomized, controlled trial in children with dilating vesicoureteral reflux. Journal of Pediatric Urology, 7(6), 594. doi: 10.1016/j.jpurol. 2011.05.006
3 Canadian Paediatric Society, (1996). Neonatal circumcision revisited. Canadian Medical Association Journal 1996: 154(6):769-780
4 Williams, N., and Kapila, L., (1993). Complications of circumcision. British Journal of Surgery; 80:1231-36.
5 Canadian Paediatric Society, (1996). Neonatal circumcision revisited. Canadian Medical Association Journal 1996: 154(6):769-780
6 Winberg, J., Bollgren, I., Gothefors, L., (1989). The prepuce: a mistake of nature? Lancet 1989; 1: 598-599
7 Canadian Paediatric Society, (1996). Neonatal circumcision revisited. Canadian Medical Association Journal 1996: 154(6):769-780
8 Canadian Paediatric Society, (1996). Neonatal circumcision revisited. Canadian Medical Association Journal 1996: 154(6):769-780
9 Denniston, G. (1996). Circumcision and the Code of Ethics. Humane Health Care International, Volume 12, Number 2: Pages 78-80.
10 Canadian Paediatric Society, (1996). Neonatal circumcision revisited. Canadian Medical Association Journal 1996: 154(6):769-780
11 Boyle, G.J., Hill, G., (2011). Sub-Saharan African randomised clinical trials into male circumcision and HIV transmission: Methodological, ethical, and legal concerns. JLM 2011;19: 316-334.
12 Storms, M.R., (1996). AAFP fact sheet on neonatal circumcision: Need for updating. Am Fam Physician 1996;54;1216,1218.
13 UNAIDS, 2002
14 Millett GA, Flores SA, Marks G, Reed JB, Herbst JH. Circumcision status and risk of HIV and sexually transmitted infections among men who have sex with men. JAMA 2008; 300:1674-1684. Errata JAMA 2009; 301: 1126-9.
15 Darby, R., Van Howe, R., (2011). Not a surgical vaccine: there is no case for boosting infant male circumcision to combat heterosexual transmission of HIV in Australia. Austr NZ J Pub Health. 2011;35(5):459-465.
16 Canadian Paediatric Society, (1996). Neonatal circumcision revisited. Canadian Medical Association Journal 1996: 154(6):769-780
September 22, 2012
Dr. Christopher L. Guest, Co-Founder of the Children’s Health and Human Rights Partnership replies to the American Academy of Pediatrics (AAP) revised statement on male infant circumcision calling it “A disservice to Americans”. His reply was published to the AAP’s on-line journal. View journal posting here.
Revised male infant circumcision policy: A disservice to Americans
The American Academy of Pediatrics (AAP) revised statement on male infant circumcision claims “the benefits of circumcision may exceed the risk of complications” but the AAP fails to recognize the sensory and mechanical function of the human foreskin. The foreskin is richly innervated, erogenous tissue which enhances sexual pleasure and it also provides a unique, linear gliding mechanism during sexual intercourse. In 2009, the College of Physicians and Surgeons of British Columbia stated “the foreskin is rich in specialized sensory nerve endings.” In 2010, the Royal Australian College of Physicians stated “the foreskin is a primary sensory part of the penis, containing some of the most sensitive areas of the penis” and in the same year, the Royal Dutch Medical Association concluded “the foreskin is a complex erotogenic structure that plays an important role in the mechanical function of the penis during sexual acts.” The AAP statement fails to consider the obstinate relationship between structure and function as it pertains to the foreskin; circumcision alters the structure of the penis which inevitably alters function. The long term harm and sexual side effects of circumcision have not been adequately studied.
The revised statement also claims “circumcision may decrease the risk of heterosexual HIV transmission” and is supported with selective evidence from randomized control trials from Kenya, Uganda and South Africa. These trials reveal a number of methodological weaknesses and they contradict larger demographic trends in global HIV prevalence. For instance, the United States has a high prevalence of circumcision, yet has a significantly higher rate of HIV infection compared with countries like Sweden and Japan where the prevalence of circumcision is very low. Behavioural factors greatly overshadow any potential protective effect of circumcision and should be the focus of effective and ethical prevention strategies. Even if the African trials were scientifically valid, the evidence can not be applied to justify infant circumcision in North America where the incidence of heterosexual HIV transmission is low.
The revised statement also claims “circumcision may decrease the risk of urinary tract infections” yet the AAP ignores the wealth of international medical evidence to the contrary. Even if circumcision provided complete protection against urinary tract infections, this practice could never be justified based on the ethical principle of proportionality – there are effective and less destructive therapies available for preventing and treating urinary tract infections which do not involve the prophylactic removal of healthy genital tissue.
The AAP’s revised statement ignores the inherent conflict of circumcision with contemporary medical ethics. Infant circumcision violates the fundamental ethical principles of autonomy, beneficence and primum non nocere. Medical associations in the Netherlands, Finland, Sweden, Norway, Denmark, Germany and other countries have stated that there is no justification for performing the procedure without medical urgency. Medical associations in these countries are calling for the practice to stop due to ethical and human rights concerns. The AAP’s new position statement does a disservice to American parents and children.
Respectfully, Christopher L. Guest M.D., F.R.C.P.C.
Conflict of Interest:
None declared
——————-
August 1, 2012
On 24 July and 01 August of 2012 representatives Tim Hammond and David Saving of the Children’s Health and Human Rights Partnership delivered a letter to the German Consulates General in Vancouver and Toronto addressed to German Chancellor Angela Merkel and the Bundestag. The letter, in both English and German, expressed CHHRP’s concern about any hasty introduction of legislation that would ‘protect circumcision’ from being prohibited. The letter urged Germany’s politicians to consider Germany’s international treaty obligations to children’s rights, as well as the impact that any such legislation would have on the rights of children not only in Germany, but in Canada and around the world.
Lesen Sie den Brief in deutscher Sprache
![]()