CORRESPONDENCE TO THE CANADIAN AIDS SOCIETY:
30 September 2013
Dear Monique Doolittle-Romas,
The Children’s Health & Human Rights Partnership (CHHRP) is Canada’s first dedicated not-for-profit partnership of medical, legal, and ethics professionals working alongside concerned citizens towards ending forced non-therapeutic genital cutting of children in Canada. We write today to share our concerns regarding your policy on male circumcision and HIV.
In particular, we ask the Canadian AIDS Society (CAS) to incorporate two issues into your male circumcision policy:
1) The methodologically flawed nature of studies that allegedly support male circumcision in the campaign against HIV
2) CAS male circumcision policy implications
Methodology
While many well-intentioned health organizations have cited the African circumcision trials as reliable evidence that male circumcision is an effective tool in the fight against HIV/AIDS, these studies are misleading. For example, assuming the quoted 50-60% risk reduction was scientifically valid, this is a “relative risk” reduction, as opposed to an “absolute risk” reduction. The absolute risk reduction in these studies was 1.31% – a significantly smaller number than the figure touted publicly.123 (Please see Appendix A for an explanation of relative and absolute risk reduction). This misleading and unscientific data manipulation falsely implies that male circumcision is effective at preventing HIV/AIDS. Many men may believe that they no longer need to use condoms after undergoing circumcision. Furthermore, these African trials contradict larger demographic trends with respect to circumcision and HIV/AIDS prevalence. For instance, the United States has a high circumcision rate but also has a significantly higher rate of heterosexual HIV transmission than other countries where circumcision is very rare. Collectable data from African countries shows circumcising countries also have a higher prevalence for HIV/AIDS, (see Appendix B). Correct and consistent use of condoms reduces HIV transmission by an absolute risk reduction of 80% 4 – far higher than the alleged 1.31% absolute risk reduction for male circumcision. Effective and ethical prevention strategies should emphasize correct condom usage, which is still required even after circumcision.
As Boyle, G. J., & Hill, G. stated, “While the ’gold standard’ for medical trials is the randomised, double-blind, placebo-controlled trial, the African trials suffered design and sampling problems including; problematic randomisation and selection bias, inadequate blinding, lack of placebo-control (male circumcision could not be concealed), inadequate equipoise, experimenter bias, attrition (673 drop-outs in female-to-male trials [7% drop out rate]), not investigating male circumcision as a vector for HIV transmission, not investigating non-sexual HIV transmission, as well as lead-time bias, supportive bias (circumcised men received additional [safe sex] counselling sessions), participant expectation bias, and time-out discrepancy (restraint from sexual activity only by circumcised men).”5 Many other scientific papers have also been highly critical of the HIV trials as a method for HIV/AIDS reduction.6789
CAS Male Circumcision Policy Implications
The CAS states in its circumcision policy statement, “Ultimately, it is another prevention option that should be available to those who choose it as such”. This begs a serious ethical and human rights question of whether the parent has the right to choose or whether consent must come from the individual to whom the genitals belong, once he reaches an appropriate age. It is the individual who must live with the permanent physical, sexual, and psychological effects of the surgery, as well as any additional surgical complications. For further information, please see the results of the Global Survey of Circumcision Harm at www.circumcisionharm.org
We receive frequent reports that many of these African circumcision programs, intended for consenting adult men, are in fact influencing North American parents to impose forced circumcision on their newborn male infants. Since these children will not become sexually active for many years, subjecting them to a permanent surgical alteration, in a misguided attempt to prevent future disease, violates their personal autonomy and robs them of their right to physical integrity as guaranteed in the Canadian Charter of Rights and Freedoms.
Canadian human rights law and treatises maintain that all children have equal protection under the law. These include:
The Universal Declaration of Human Rights (UDHR), adopted by Canada in 1948 (http://www.un.org/en/documents/udhr/)
The United Nations Convention on the Rights of the Child (CRC) ratified by Canada in December 1991. Specifically, Article 24.3 declares, “State Parties shall take all effective and appropriate measures with a view to abolishing traditional practices prejudicial to the health of children.” (http://www.un.org/documents/ga/res/44/a44r025.htm)
The Canadian Charter of Rights and Freedoms, enshrined in the Canadian constitution in 1982 (http://laws-lois.justice.gc.ca/eng/Const/page-15.html)
Any form of non-consensual female genital cutting—equal to or less invasive than male infant circumcision, including removal of the female prepuce—for any reason, including the potential to reduce vulvar cancer or sexually transmitted diseases, has been illegal in Canada since 1997.1011 Circumcision of otherwise normal healthy boys is in direct conflict with gender equality rights spelled out in the above documents.
The Valid Function of the Foreskin
“The prepuce [foreskin] is an integral, normal part of the external genitalia that forms the anatomical covering of the glans penis and clitoris… The prepuce is richly innervated, erogenous tissue.”12 It also serves an important mechanical function, providing a linear bearing mechanism during sexual intercourse.1314 For further information on the form and function of the penis and the mechanics of intercourse please visit the cited references.
Respect for a child’s developing sexuality, regardless of gender, is recognized in the 1997 Valencia Declaration of Sexual Rights adopted by the XIII World Congress of Sexology, which states:
“We urge that societies create the conditions to satisfy the needs for the full development of the individual and respect the following sexual rights: …The right to autonomy, integrity and safety of the body. This right encompasses control and enjoyment of our own bodies, free from torture, mutilation and violence of any sort.”15
Summary
CHHRP invites the CAS to join thousands of people around the world in efforts to define, expand, and protect human rights in health relevant settings—such as sexual rights and health—and to uncover substantial inconsistencies in health thinking. One such inconsistency is the unquestioned respect for a female child’s right to genital integrity and autonomy that has thus far been ignored for the male child.
It is our hope that the CAS will recognize that male circumcision is not an effective tool in the fight against HIV/AIDS. We also hope that the CAS recognizes the human rights and possible Canadian legal implications of suggesting male circumcision as part of a HIV/AIDS prevention strategy. We look forward to a continuing dialogue with the CAS.
Respectfully submitted by,
Christopher L. Guest M.D., F.R.C.P.C.
Medical Director, Children’s Health & Human Rights Partnership
1300 King St E PO Box 31011
Kingsway Village PO
Oshawa, ON L1H 8N9
References
1 Bailey, R.C., Moses, S., Parker, C.B., Agot, K., Maclean, I., Krieger, J.N., et al. Male circumcisi1on for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet 2007; 369: 643-56 doi: 10.1016/S0140-6736(07)60312-2 pmid: 17321310.
2 Auvert, B., Taljaard, D, Lagarde, E., Sobngwi‐Tambekou, J., Sitta, R., & Puren, A. (2005). Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: the ANRS 1265 Trial. PLoS medicine, 2 (11), e298.
3 Gray, R. H., Kigozi, G., Serwadda, D., Makumbi, F., Watya, S., Nalugoda, F., et al. (2007). Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. The Lancet, 369 (9562), 657‐666.
4 Wilton, J. (2013). Condoms: Tried, tested and true? From CATIE: Canada’s source for HIV and hepatitis C information:http://www.catie.ca/pif/spring‐2013/condoms‐tried‐tested‐and‐true
5 Boyle, G. J., & Hill, G. (2011). Sub‐Saharan African randomised clinical trials into male circumcision and HIV transmission: methodological, ethical and legal concerns. Journal of law and medicine, 19 (2), 316.
6 Green, et al., (2010). Male Circumcision and HIV Prevention: Insufficient Evidence and Neglected External Validity. Am J Prev Med 2010;39(5):479–482
7 Darby, R. & Van Howe, R. (2011), Not a surgical vaccine: there is no case for boosting infant male circumcision to combat heterosexual transmission of HIV in Australia. Australian and New Zealand Journal of Public Health, 35: 459–465. doi: 10.1111/j.1753‐ 6405.2011.00761.x
8Frisch, M., Aigrain, Y., Barauskas, V., Bjarnason, R., Boddy, S. A., Czauderna, P., et al. (2013). Cultural bias in the AAP’s 2012 technical report and policy statement on male circumcision. Pediatrics , 131 (4), 796‐800.
9Van Howe, R. S. & Storms, M. R. (2011). How the circumcision solution in Africa will increase HIV infections. Journal of Public Health in Africa 2011; 2:e4 doi: 10.4081/jphia.2011.e4
10 Government of Canada. (2013, July 15). Justice Laws Website. From Criminal Code s 266 Assault: http://laws‐lois.justice.gc.ca/eng/acts/C‐46/page‐131.html#docCont
11Parliament of Canada. (n.d.). BILL C‐27. From Parliament of Canada:http://www.parl.gc.ca/HousePublications/Publication.aspx?DocId=2329459&File=16
12 Cold, C. J., & Taylor, J. R. (1999). The prepuce. BJU international , 83 (S1), 34‐44.
13 Anatomy of the Penis, Mechanics of Intercourse (http://www.cirp.org/pages/anat/)
14 Animation on the foreskin linear bearing mechanism during sexual intercourse (http://www.circumstitions.com/Works.html)
15 World Association for Sexology. (2007, November). Valencia Declaration on Sexual Rights.
Appendix A
WHAT DOES RELATIVE RISK REDUCTION AND ABSOLUTE RISK REDUCTION MEAN?
The misleading Relative Risk Ratio
Newspapers like big numbers and eye-catching headlines. They need miracle cures and hidden scares, and small percentage shifts in risk will never be enough for them to sell readers to advertisers (because that is the business model). To this end they pick the single most melodramatic and misleading way of describing any statistical increase in risk, [Or “Reduction” in the case of circumcision and HIV] which is called the ‘relative risk increase’.
Let’s say the risk of having a heart attack in your fifties is 50 per cent higher if you have high cholesterol. That sounds pretty bad. Let’s say the extra risk of having a heart attack if you have high cholesterol is only 2 per cent. That sounds OK to me. But they’re the same (hypothetical) figures. Let’s try this. Out of a hundred men in their fifties with normal cholesterol, four will be expected to have a heart attack; whereas out of a hundred men with high cholesterol, six will be expected to have a heart attack. That’s two extra heart attacks per hundred. Those are called ‘natural frequencies’.
Natural frequencies are readily understandable, because instead of using probabilities, or percentages, or anything even slightly technical or difficult, they use concrete numbers, just like the ones you use every day to check if you’ve lost a kid on a coach trip, or got the right change in a shop. Lots of people have argued that we evolved to reason and do maths with concrete numbers like these, and not with probabilities, so we find them more intuitive. Simple numbers are simple.
The other methods of describing the increase have names too. From our example above, with high cholesterol, you could have a 50 per cent increase in risk (the ‘relative risk increase’); or a 2 per cent increase in risk (the ‘absolute risk increase’); or, let me ram it home, the easy one, the informative one, an extra two heart attacks for every hundred men, the natural frequency.
As well as being the most comprehensible option, natural frequencies also
contain more information than the journalists’ “relative risk increase”.
Excerpt from “Bad Science” by Ben Goldacre, Fourth Estate, London (2008), p 256-9
Appendix B
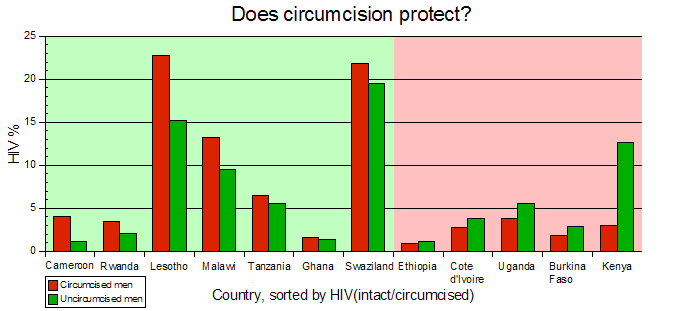
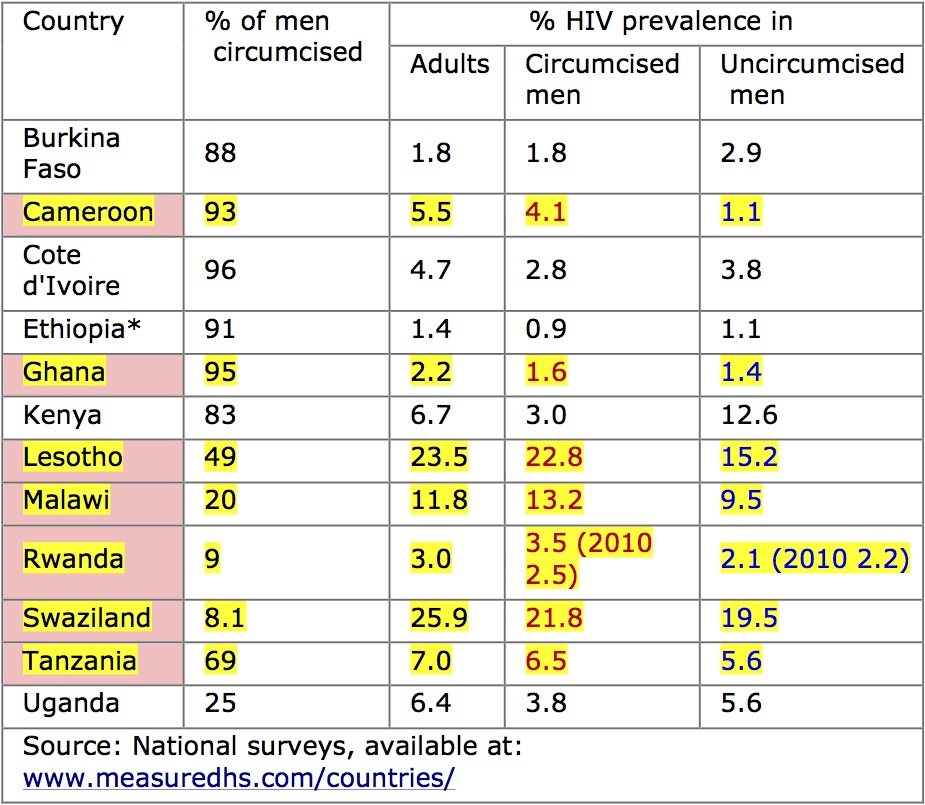
Male circumcision and HIV prevalence in Africa
“There appears to be no clear pattern of association between male circumcision and HIV prevalence. In 8 of 18 countries with data, as expected, HIV prevalence is lower among circumcised men, while in the remaining 10 countries HIV prevalence is higher among circumcised men…
Findings from the 18 countries with data present a mixed picture of the association between male circumcision and HIV prevalence. In eight of the countries (Burkina Faso, Cambodia, Côte d’Ivoire, Ethiopia, Ghana, India, Kenya, and Uganda), HIV prevalence is higher among men who are not circumcised, although the difference between circumcised and non-circumcised men is slight, except in Kenya, where the difference is substantial (HIV prevalence of 11.5 percent for non-circumcised men compared with 3.1 percent for circumcised men). In 10 of the countries (Cameroon, Guinea, Haiti, Lesotho, Malawi, Niger, Rwanda, Senegal, Tanzania, and Zimbabwe) HIV prevalence is higher among circumcised men.”
United States Agency for International Development (USAID) February 2009